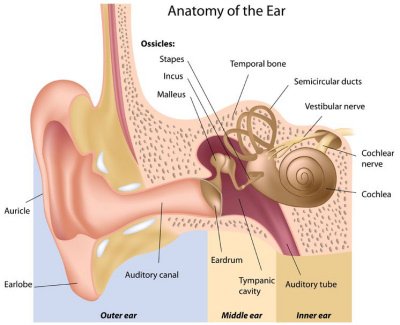
-Acute Otitis Media-

-Acute Otitis Media-
-clinical diagnosis of acute otitis media requires a bulging tympanic membrane or other signs of acute inflammation and middle ear effusion
-comes usually from an antecedent event such as a viral URI with a colonized bacteria in middle ear, this results in inflammatory edema in the respiratory mucosa of nose, pharynx and eustachian tubes and this obstructs the drainage of the tubes.
-usual pathogens are Strep Pneumonia, Haemophilus influenza, and Moraxella Catarrhalis
-with antibiotic therapy typically symptoms and signs resolve themselves within 24-72 hours
-treated with analgesics ibuprofen or acetaminophen. Topical benzocaine preparations are alternatives for ear drops except with perforation
-children less than 2 years of age should be treated with antibiotics regardless
-children greater than 2 years who appear toxic, have an earache for over 2 days, have a temperature over 102.2 in the last 48 hours should be treated with antibiotics
-in addition children with bilateral otitis media or otorrhea should be given antibiotics
-first line therapy is amoxicillin
-augmentin first line if there children have increased risk of beta lactam resistance, antibiotic in the last 30 days or have an concomitant conjunctivitis
-macrolides or cefuroxime, or cefpodoxime, or rocephin are an alternative for those with allergy or hypersensitivity
-Indications for tympanostomy tubes-
-otitis media effusion who are at risk of speech, language or learning problems
-persistent otitis media with effusion with a hearing loss over 40 decibels
-bilateral otitis media for greater than 3 months or unilateral otitis media for greater than 6 months
-recurrent episodes of otitis media with a cumulative duration of greater than 6 months over a 24 month span.
-Chronic Otitis Media-
-it is a recurrent infection of the middle ear and/or mastoids in the presence of tympanic membrane perforation
-usually have decreased acoustic acuity, otorrhea, otalgia, and may have vertigo
-Cholesteatoma, keratinized tissue in the middle ear or mastoid, can occur as a primary lesion or secondary to tympanic membrane perforation
-chronic serous otitis media is characterized by continuous serous drainage that is straw colored
-duration is controversial ranging from 2 weeks to 3 months
-usually comes from eustachian tube dysfunction (URI or allergic rhinitis)
-pseudomonas and staphylococcus aureus are the most common isolated organisms. Fungi can cause
-treatment is focused at stopping otorrhea, healing tympanic membrane and eradicating infection
-topical antibiotic are first line treatment with uncomplicated otorrhea, topical floxacin or vigamox
-systemic antibiotics should be considered for patients at risk for invasive ear infections or failed therapy with topical antibiotics. Imipenem is the most effective
-may require surgery if above fails
-Acoustic Neuroma-

-also known as vestibular schwannoma
-these are tumors that arise from the vestibular portion of CN VIII
-symptoms associated can be due to cranial nerve involvement, cerebellar compression or tumor progression
-major symptoms include hearing loss, tinnitus, unsteady gait, true vertigo is uncommon
-trigeminal nerve impingement can cause paresthesia, pain, and hyperesthesia
-facial nerve impingement can cause facial paresis, and taste disturbances
-large tumors can but pressure on the posterior fossa and adjacent structures causing ataxia
-bilateral acoustic neuromas should lead clinician to suspect neurofibromatosis
-MRI is the imaging study of choice
-treatment options are surgery, radiation, and observation
-Barotrauma-

-pressure can be increased with eustachian tube dysfunction or something obstructing the eustachian tube
-the pressure differences distort the tympanic membrane and can cause discomfort, hearing loss or perforation
-eustachian tube dysfunction etiologies include URI, otitis media, or allergic rhinitis
-barotrauma can happen from flying, diving, or blast injuries
-presenting symptoms and signs are pressure in the ear, hearing loss may occur
-may cause vertigo or tinnitus
-best treatment is prevention. Analgesic can help. Antihistamines, nasal sprays decongestant may help decrease obstruction from the eustachian tube
-antibiotics orally should only be used with the middle ear is contaminated with perforation
-Cholesteatoma-
-patients may be asymptomatic or have combinations of hearing loss, dizziness, or otorrhea
-diagnosis is made by visualization
-gram stains and cultures should be obtained if they fail standard topical therapy
-if there is no response to medical therapy biopsy should be obtained
-Eustachian Tube Dysfunction-

-eustachian tube dysfunction is a failure of the functional valve of the eustachian tube to open and or close properly
-eustachian tube dysfunction can come from pressure dysregulation, impaired protective function, and diminished clearance
-functional obstruction is most commonly from mucosal inflammation with edema and secretions inhibiting valves ability to open and close
-there can be negative pressure within the eustachian tube from usual circumstances of diving or air travel
-a dull bluish gray or yellowish discoloration can denote an effusion
-can tray decongestants and nasal spray but no study has demonstrated consistent efficacy
-surgery is only indicated when medical management fails
-Ear Foreign Body-

-successful removal of foreign bodies requires appropriate local anesthesia or may even require procedural sedation for more difficult foreign bodies
-local anesthesia mainly necessary for removing foreign bodies from the pinna
-proper restraint, good lighting, and appropriate instruments are needed for removal
-infection of the cartilage should be treated with antibiotics. Pseudomonas is the main pathogen. MRSA should also be considered. Cipro in adults. Parenteral antibiotics with vancomycin or clindamycin and cefiazidime)
-insects in the EAC should be killed with mineral oil, ethanol, or lidocaine prior to removal
-can irrigate ear for smaller objects unless tympanostomy tubes or perforated tympanic membrane or removal of vegetable matter or button batteries
-can try to remove with mosquito forceps under direct visualization
-have low threshold for referral to ENT especially for high risk for TM perforation or EAC laceration
-Hearing Impairment-

-Hearing loss is classified into 3 types: sensorineural, conductive, or mixed
-Sensory: involves the inner ear, cochlea, or the auditory nerve
-Conductive: involves limiting the amount of external sound gaining access to the inner ear (cerumen impaction, middle ear effusion, or lack of movement of the small bones of the inner ear
-Mixed: a combination of sensory and conductive hearing loss
-Weber Test-pressing the handle on the tuning fork to the bridge of the nose, forehead, or teeth and asking the patient if the sound is louder in one ear than the other
-Weber test is normal if heard in both ears equally
-Rhinne test- tunning fork is placed on mastoid bone versus when it is held near the ear. Its abnormal when the sound is at least equally loud or louder when the fork is placed on the bone as compared when it is by the ear (bone>air conduction)
-Rhinne test normal when the air conduction > bone conduction
-Weber and Rhinne help decide if sensory or conductive hearing loss
-Weber test the sound is louder on the good side and less on the bad side (conductive hearing loss)
-If the Weber test goes to an ear and the Rhinne is normal, and if there is a normal Rhinne test in the other ear, sensory hearing loss is implied. Audiogram should be preformed.
-If had conductive hearing loss, should have otoscopy to determine if cerumen impaction or reason for conductive hearing loss
-Etiologies of hearing loss: congenital, trauma, infection, tumor, exostosis, polyps, osteoma, cerumen, systemic disease, and dermatologic (psoriasis can cause scaling and edema of the EAC and meatus), ototoxic ingestion of substances
-Presbycusis- age related hearing loss
-Hearing aids helpful for bilateral sensory hearing loss or long term conductive hearing loss
-Cochlear implants are good for children with profound bilateral hearing loss who do not benefit from traditional amplification
-Surgery is indicated for surgically correctable causes
-Hematoma of the External Ear-

-ear hematomas typically comes from blunt trauma during sports
-this injury requires prompt drainage to his ear and measures to prevent reaccumulation of blood
-cauliflower ear is the permanent deformity caused by fibrocartilage overgrowth that occurs when an auricular hematoma is not fully drained or reoccurs
-all auricular hematomas should be drained as soon as possible after the injury
-Labyrinthitis-
-labyrinthitis is characterized by a sudden onset of severe, persistent vertigo, nausea, vomiting and gait problems.
-on physical exam there is vestibular imbalance, nystagmus, and a positive head thrust
-there is unilateral hearing loss with this. If there is no hearing loss it is vestibular neuritis
-it is a post viral inflammatory disorder of the eighth cranial nerve
-clinical features of cerebellar infarction or bleeding are similar so brain MRI or CT is required to rule out
-can treated vertigo with antivert, Ativan or valium
-condition will be self limiting
-physical therapy can help preserve vestibular function
-Mastoiditis-

-acute mastoiditis is the most common suppurative complication of otitis media
-it is defined as a suppurative infection of the mastoid air cells
-defines as acute if it is less than one month in duration
-most common pathogen is Streptococcus pneumoniae
-pseudomonas should be considered for recurrent with recurrent otitis media and ruptured tympanic membrane
-antibiotic therapy and drainage of the middle ear and mastoids are cornerstones of therapy
-vancomycin and cefazidime are recommended for empiric therapy for mastoiditis
-diagnosis can be confirmed with CT scan or MRI
-Meniere's Disease-

-syndrome causing episodic vertigo, tinnitus, and hearing loss
-usually presents between the ages of 20-40
-it is associated with endolymphatic hydrous and distention of the labyrinthine system
-clinical diagnosis. Definitive diagnosis is only made postmortem
-MRI indicated to rule out CNS etiology that may mimic Meniere's disease
-management is geared at improving quality of life and management of symptoms
-anti-emetics and antivert helps with symptoms. Valium or ativan can help with vertigo also
-Otitis Externa-
-otitis externa refers to inflammation of the external auditory canal
-can be infectious, allergic, or dermatologic related
-also called swimmers ear
-risk factors include swimming or other water exposure, trauma from aggressive cleaning, wearing ear devices
-allergic contact dermatitis can lead to otitis externa
-dermatologic conditions such as psoriasis or atopic dermatitis can can cause otitis externa
-Staphylococci are the most common organisms
-Clinical features of otitis externa are ear pain, purulent drainage, discharge and hearing loss
-there is pain with movement of the tragus and or pinna
-rarely can be fungal in etiology
-cultures are reserved for patients with severe otitis externa
-the removal of cerumen, desquamated skin and purulent material aids in the penetration of the drops
-Cipro and Oflaxacin ear drops are excellent and provide coverage of the main pathogens staph aureus and psuedomonas
-Cortisporin provides great coverage also
-wick placement is for when canal is swollen shut to allow for better penetration of drops
-Tinnitis-
-Tinnitus is the perception of sound in proximity to the head in the absence of an external source
-Can be in one or both ears
-Tinnitus can be described as a ringing, hissing or buzzing
-Can be continuous or intermittent
-Can be triggered anywhere along the auditory pathway
-Most patients have sensorineural tinnitis due to hearing loss at the cochlear nerve level
-Pulsatile tinnitus is most commonly due to a vascular etiology
-arterial bruits near the temporal bone may transmit sounds and cause tinnitus
-congenital AV malformations can be associated with hearing loss or tinnitus
-paragangliomas are benign tumors that can cause tinnitus
-Venous hums from systemic hypertension and increased ICP (sometimes due to pseudotumor cerebri) can cause conductive hearing loss and cause tinnitus
-eustachian tube dysfunction can cause tinnitus and also somatic disorders
-also ototoxic medications and vestibular schwannoma (tumor compressing on cochlear nerve)
-treatment of tinnitus involves treating or correcting the etiology
-Tympanic Membrane Perforation-
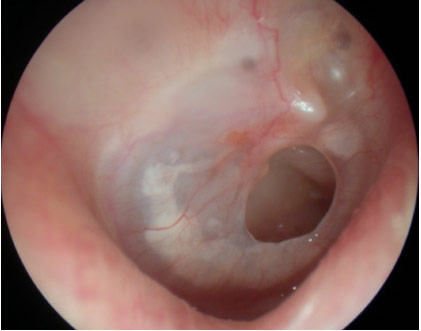
-perforated tympanic membranes are caused by middle ear infections, barotrauma, or the patient is poked with a sharp object
-patients can range from no symptoms to, ear pain, ear pain that quickly resolves, otorrhea, tinnitus, or hearing loss
-treatment involves oral and topic ear antibiotic drops if caused by an infection
-usual treat involves amoxicillin and floxin ear drops and analgesics
-should be referred to ENT to make sure TM heals properly
-need to wear ear plugs to ensure no water makes it into the middle ear when showering or bathing
-Vertigo-

-Vertigo is a symptom that the patient is moving. It is a sense of swaying, tilting, or spinning
-Vertigo happens because of asymmetry of the vestibular system due to damage of the labyrinth, vestibular nerve, or central vestibular structures of the brainstem
-Benign Paroxysmal Positional Vertigo -tends to have recurrent brief episodes of vertigo, predictable with head movements or positions, will have no auditory symptoms and have a positive Hallpike maneuver
-Vestibular Neuritis- usually has a single episode that last for days, viral syndrome may accompany or precede symptoms, nystagmus fall toward the side of lesion. Head thrust is abnormal
-Meniere's Disease-has recurrent episodes that last several minutes to hours. This has episodes of ear fullness or pain with unilateral hearing loss or tinnitis.
-Migranous Vertigo-will have recurrent episodes last several minutes to hours, history of migraine, may have a nystagmus with central or peripheral characteristics. Tests are usually normal
-Vestibular TIA-single episode lasting minutes to hours, central nystagmus, usually older patient, MRI may show lesion
-Cerebellar Infarction or Hemorrhage-sudden onset of symptoms over days to weeks, older patient, central nystagmus, trouble walking, CT/MRI will show lesion
-history and physical is the best tool for determine the etiology, but imaging is required to exclude life threatening or more severe causes.
-Treatment is directed at determining the etiology. If correctable cause, it needs to be corrected.
-Antivert, valium or ativan good for managing vertigo on as needed basis.
-May need physical therapy if debilitating symptoms
No comments:
Post a Comment